InBra™ Electric
Hands-free breast pumps with in-bra collection cups and a rechargeable battery for easy multi-tasking. Available in single or double cups.

Hands-free Electric
Explore Medela's hands-free electric breast pumps with in-bra collection cups and rechargeable battery. Pump while you multitask. Discover more now!

Classic Electric
Discover Medela's electric breast pumps with 2-Phase Expression technology. Express more milk efficiently and quickly. Explore our advanced pumps today!

Manual
Explore Medela's single manual breast pumps. Ideal for occasional use and lightweight for easy travel. Find your perfect pump today!

Symphony - No 1 Hospital Pump
Explore the Medela Symphony® breast pump—perfect for hospitals and home use with reliable, multi-user performance. Learn more now!


Pumping garments
Find Medela's Pumping Bra and Bustier for easy breastfeeding and pumping. Enjoy comfort and convenience with designs made for busy moms. Learn more!

Maternity & nursing bras
Explore Medela’s maternity bras and bralettes for nursing, crafted for comfort and easy breastfeeding. Ideal for new and expectant mothers. Learn more now!

Bottles & Bags
Need breast milk bottles & bags? Medela provides breast milk storage bottles, and storage bags for easy and effective milk storage.

Hospital-only products
The breastfeeding specialist Medela offers a wide range of products for hospital use that make breast milk feeding more simple and comfortable





Connectors
Find Medela's connectors for your breast pump to ensure seamless operation and efficient pumping. Get the extra parts you need. Learn more now!

Membranes
Find Membranes for Medela Hands-Free and Symphony Pumps. Replace worn parts to maintain pump efficiency and comfort. Explore options now!
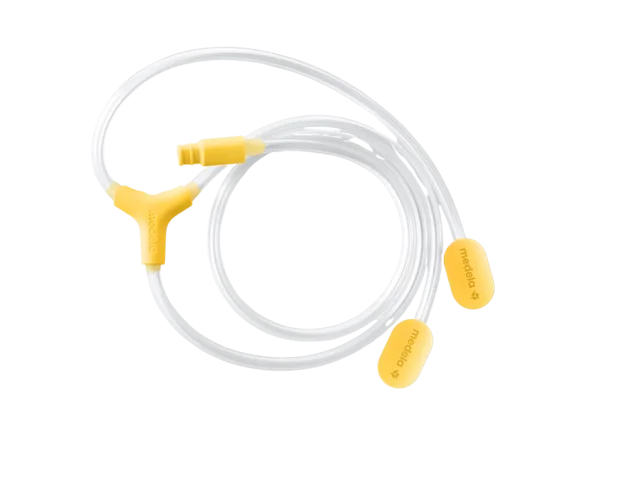
Tubing
Explore Medela’s durable breast pump tubing for reliable, efficient milk expression. Easy to clean and replace. Learn more now!

Shields
Explore Medela's breast shields for comfort and efficiency. Enhance your pumping experience with our high-quality options. Learn more now!

Power units
Find reliable breast pump power adapters from Medela for consistent performance. Upgrade or replace your unit easily. Learn more now!

Hands-free Set




















InBra™ Electric
Hands-free breast pumps with in-bra collection cups and a rechargeable battery for easy multi-tasking. Available in single or double cups.
Hands-free Electric
Explore Medela's hands-free electric breast pumps with in-bra collection cups and rechargeable battery. Pump while you multitask. Discover more now!
Classic Electric
Discover Medela's electric breast pumps with 2-Phase Expression technology. Express more milk efficiently and quickly. Explore our advanced pumps today!
Manual
Explore Medela's single manual breast pumps. Ideal for occasional use and lightweight for easy travel. Find your perfect pump today!
Symphony - No 1 Hospital Pump
Explore the Medela Symphony® breast pump—perfect for hospitals and home use with reliable, multi-user performance. Learn more now!
Pumping garments
Find Medela's Pumping Bra and Bustier for easy breastfeeding and pumping. Enjoy comfort and convenience with designs made for busy moms. Learn more!
Maternity & nursing bras
Explore Medela’s maternity bras and bralettes for nursing, crafted for comfort and easy breastfeeding. Ideal for new and expectant mothers. Learn more now!
Bottles & Bags
Need breast milk bottles & bags? Medela provides breast milk storage bottles, and storage bags for easy and effective milk storage.
Hospital-only products
The breastfeeding specialist Medela offers a wide range of products for hospital use that make breast milk feeding more simple and comfortable
Connectors
Find Medela's connectors for your breast pump to ensure seamless operation and efficient pumping. Get the extra parts you need. Learn more now!
Membranes
Find Membranes for Medela Hands-Free and Symphony Pumps. Replace worn parts to maintain pump efficiency and comfort. Explore options now!
Tubing
Explore Medela’s durable breast pump tubing for reliable, efficient milk expression. Easy to clean and replace. Learn more now!
Shields
Explore Medela's breast shields for comfort and efficiency. Enhance your pumping experience with our high-quality options. Learn more now!
Power units
Find reliable breast pump power adapters from Medela for consistent performance. Upgrade or replace your unit easily. Learn more now!
Hands-free Set
Pump In Style® Pro+ Hands-free Rechargeable Breast Pump
Power meets portability. Pump In Style Pro+ delivers clinically proven performance in a compact, lightweight design built for your lifestyle.
Purelan™ lanolin cream
In the first few days and weeks of frequent breastfeeding, many women experience nipple soreness and dry skin. Purelan™ lanolin cream gives you fast relief for sore nipples and dry skin.

Symphony PLUS® breast pump
Engineered with Initiation Technology™ proven to help mothers initiate, build, and maintain their breast milk supply